

Background: Multiple myeloma is a heterogenous plasma cell cancer characterized by expression of a monoclonal protein (M-protein) or free light chains (FLC). Although survival has improved over the past 15 years, outcomes are variable and not fully predicted by conventional prognostic markers. Survival is associated with depth and duration of response to treatment but it is not known if the trajectory of response is associated with survival.
We hypothesized that the trajectory of M-protein over the first six months of treatment in patients with newly diagnosed multiple myeloma can identify distinct clinical groups and is an independent predictor of overall survival (OS). The objectives of our study are to: 1) Identify groups of patients with different M-protein trajectories using trajectory analysis; 2) Evaluate patient and illness factors associated with different M-protein trajectories; and 3) Determine whether M-protein trajectory is an independent predictor of OS in newly diagnosed multiple myeloma.
Methods: We conducted a retrospective cohort review of all patients with newly diagnosed multiple myeloma in Manitoba between 2012 and 2017 who had a measurable M-protein at presentation and who were initially treated with bortezomib-based chemotherapy. Baseline characteristics and monthly response assessments up to six months were collected and analyzed using trajectory analysis. We used latent class mixed models (LCMM) to produce trajectory groups of M-protein response over time. We used the Bayesian Information Criterion and clinical validity characteristics to select the optimal trajectory model. We developed a multinomial logistic model to evaluate the association of patient and illness characteristics with M-protein trajectories. We constructed a multivariable Cox proportional hazard model adjusted for trajectory group, ISS stage, transplant status, LDH, renal failure and platelet count to evaluate the association of M-protein trajectory on OS in multiple myeloma.
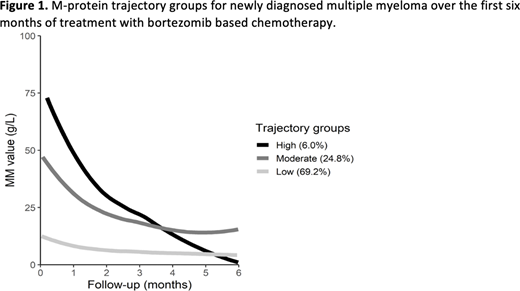
Results: 266 patients were included in the trajectory analysis. 154 (57.9%) were male. Mean age was 66.4 years (SD 10.1). 29 (10.9%) were classified as ISS stage 1, 80 (30.1%) as ISS stage 2, and 109 (41.0%) as ISS stage 3. The best fit trajectory model identified three trajectory groups representing distinct M-protein trajectories over time (Figure 1). We plotted the trajectory of the absolute value for M-protein as the percentage change from baseline did not separate the population into distinct groups. Baseline bone marrow plasma percentage (p<0.01), albumin (p<0.01), and hemoglobin (p<0.01) were significantly associated with trajectory group membership. The median follow-up was 2.74 years for the OS analysis. The median OS was not reached for the low group, 4.3 years for the moderate group, and 5.4 years for the high group. In a multivariable Cox proportional hazard model, we found that trajectory group was not significantly associated with OS (moderate group HR 1.18, 95%CI 0.48-2.91, high group HR 1.10, 95%Cl 0.62-1.88). Variables significantly associated with OS included ISS stage (p<0.025), LDH (p<0.022), platelet count (p<0.001), and receipt of a stem cell transplant (p<0.001).
Discussion and Conclusions: In this retrospective cohort study of patients with newly diagnosed multiple myeloma, we identified three distinct groups based on their M-protein trajectory over time. The identified groups have different mean baseline M-protein values and follow different evolutionary patterns over time. While M-protein trajectory group was not associated with differences in OS, the small sample size and short follow-up may limit interpretation of the results. Our analyses only looked at the M-protein trajectory over the first six months after treatment start, which indicates an early response to treatment. It is possible this early response does not play a large role in the OS of patients with myeloma given the mutliple lines of chemotherapy they may receive. Further studies are planned to assess the achievement of a complete remission at one year or at renal recovery for patients affected with renal involvement. Alternative uses for M-protein trajectory analysis include the trajectory of M-protein prior to relapse or in patients with smoldering myeloma to identify who may benefit from earlier treatment.
Kotb:Takeda: Honoraria; Merck: Honoraria, Research Funding; Sanofi: Research Funding; Celgene: Honoraria; Janssen: Honoraria; Amgen: Honoraria; Karyopharm: Current equity holder in publicly-traded company.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal